


|
Rescooped by Lionel Reichardt / le Pharmageek from Digital Pharma news |


No comment yet.
Sign up to comment
Get Started for FREE
Sign up with Facebook Sign up with X
I don't have a Facebook or a X account


 Your new post is loading...
Your new post is loading... Your new post is loading...
Your new post is loading...
No comment yet.
Sign up to comment
FDA said it will ease up vetting general health and wellness apps, but it will scrutinize clinical applications and devices. Does this mean the FTC will step up?
The U.S. Food and Drug Administration has issued final guidance on “low-risk” digital health apps and devices for general health management 18 months after it came out with draft guidance. The document offers information on the kinds of apps and devices for which it will and won’t take action. Apps promoting or maintaining a healthy weight or to assist with weight loss goals and healthy eating are OK. The guidance says that companies can make claims that their apps and devices can help with healthy lifestyle choices to reduce the risk of chronic conditions such as Type 2 diabetes, high blood pressure and heart disease or improve their management. But those lifestyle choices have to be advocated by the likes of the American Heart Association or American Association of Clinical Endocrinologist or peer-reviewed medical journals. So what are some examples of what’s not OK? Claims that a product will treat or diagnose obesity, an eating disorder, such as bullimia or anorexia, or an anxiety disorder. Digital health entrepreneurs are also encouraged to ask themselves the following questions: Is the product invasive? If the answer is yes to any of the above, they need to assume their products are considered clinical applications, will be scrutinized and should act accordingly. My takeaway from the guidance is twofold. It’s a question of resources. Although there are thousands of general wellness apps, more and more medical device and pharma companies are developing digital health devices and apps of their own. Second, the Federal Trade Commission has shown it is willing to take action against companies that it deems to be making false health claims about their apps and devices.
Via rob halkes

rob halkes's curator insight,
August 1, 2016 4:50 AM
Health apps should do what they promise! At the moment they need to take a diagnostic feature and use personal physics to arrive at advice or conclusions about the health status of the person who uses the app, they are considered not to be 'just' an "app" but a medical device. At that condition they need to adhere to and be certified by several criteria attached to 'medical devices". Developers should know about this, which the more professional ones will. Rightly so! PatientView has developed a website MyHealthApps that presents an inventory of the better Health Apps. 
Pharma Guy's curator insight,
August 1, 2016 8:38 AM
Also read “FDA Won't Regulate ‘Low-Risk’ mHealth Apps as Medical Devices. But Battle Looms Over Defining ‘Low Risk’"; http://sco.lt/5kkDyr

The Food and Drug Administration (FDA), which regulates everything from heart monitors to horse vaccines, will soon have its hands full with consumer health apps and devices.
The vast majority of the health apps you’ll find in Apple’s or Google’s app stores are harmless, like step counters and heart beat monitors. They’re non-clinical, non-actionable, and informational or motivational in nature.
But the next wave of biometric devices and apps might go further, measuring things like real-time blood pressure, blood glucose, and oxygen levels. More clinical apps The FDA is charged with keeping watch on the safety and efficacy of consumer health products. Lately, that includes more clinical apps as well as devices you might buy at the drugstore, like a home glucose testing kit.
“It’s these apps that the FDA says it will regulate,” David Bates of Brigham and Women’s Hospital and Physicians Organization told VentureBeat in June. These apps will have to go through the full 510(k) process,” he said.
Dr. Bates chaired a group to advise the FDA on how to review health apps for approval, and on how the FDA should advise developers. “It was intended to help them think through the risk factors involved with these products and then give guidance on how to stay within the guidelines,” he said.
“The device makers were asking from some guidance from The FDA on what types of things would be accepted and what wouldn’t,” Bates said. Bates believes the FDA wants to use a light regulatory touch when looking at new medical devices. “The FDA definitely wants innovation to continue in clinical devices,” he said. “In general the FDA knows that the vast majority of apps are just informational.”
The FDA’s final guidance focuses on a small subset of mobile apps that present a greater risk to patients if they do not work as intended.
Health apps go mainstream The big software companies (Apple, Google, and Samsung) have brought attention to, and lent credibility to, apps and devices that do more than count steps. These companies are building large cloud platforms designed to collect health data from all sorts of health apps and devices.
more at http://venturebeat.com/2014/07/21/health-apps-are-changing-so-must-the-fda/
Via nrip, Clara Hamelin

The FDA is creating a largely automated surveillance system to monitor safety of high-risk medical devices, and has authorized a cellphone app for doctors to simplify reporting deaths and injuries to the agency. Via Seth Bilazarian, MD, Lionel Reichardt / le Pharmageek

Seth Bilazarian, MD's curator insight,
April 24, 2013 4:25 PM
"There's an app for that." Physicians are often criticized for not doing a better job reporting adverse events and this is largely because the method for reporting to the FDA has been burdensome and difficult. An easy to use reporting strategy from a smartphone will increase my reporting dramatically. The speed of reporting and analysis by FDA for actionable items should be significantly shortened.
Seth Bilazarian, MD's comment,
April 24, 2013 4:27 PM
#app, medical app, #chealth, #mHealth, FDA, adverse event reporting, Bilazarian
|
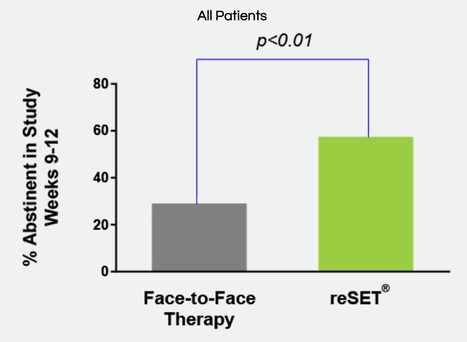
US regulators have approved the first mobile medical application for substance use disorders involving alcohol, cocaine, marijuana and stimulants.
Via Pharma Guy, Giuseppe Fattori
Pharma Guy's curator insight,
September 15, 2017 7:56 AM
When I first saw this story, I thought this app also helped patients who are addicted to opioids. I wonder if anything could solve that problem! 
Richard Platt's curator insight,
September 29, 2017 10:40 PM
The FDA’s approval came on the back of a 12-week clinical trial involving 399 patients on either standard treatment or standard treatment plus a desktop version of Reset. It showed a statistically significant increase (40.3% vs 17.6%) in adherence to abstinence for patients with alcohol, cocaine, marijuana and stimulant SUD who used Reset. The trial did not demonstrate the effectiveness of using Reset for opioid abuse and the application is not licensed to treat opioid dependence. Carlos Peña, director of the Division of Neurological and Physical Medicine Devices in the FDA’s Center for Devices and Radiological Health, said: “This is an example of how innovative digital technologies can help provide patients access to additional tools during their treatment. “More therapy tools means a greater potential to help improve outcomes, including abstinence, for patients with substance use disorder.” Reset contains a patient application and clinician dashboard and is indicated as a prescription-only adjunct treatment for patients with SUD who are not currently on opioid replacement therapy, do not abuse alcohol solely or whose primary substance of abuse is not opioids. However, Pear’s development pipeline does include a version of the app specifically for opioid use disorder, alongside devices for use in areas such as schizophrenia, pain and major depressive disorder.

You’re developing a health app for mobile devices and you want to know which federal laws apply. Check out this interactive tool.
Via Pharma Guy, Giuseppe Fattori
Pharma Guy's curator insight,
April 16, 2016 6:59 AM
Related: "An Analysis of Genentech's 4HER Mobile Health App Privacy Policy"; http://bit.ly/4HERapp and "mHealth App Developers Ask for HIPAA Clarity"; http://bit.ly/mAppHIPAA I used this tool thinking of a few pharma mHealth apps I have seen. To see the results of that exercise, click here: http://bit.ly/mHealthAppQandA

Why clinical trials need mobile health tools .. CROs (clinical research organization, "an organization that provides support to the pharmaceutical and biotechnology industries in the form of research services outsourced on a contract basis") as we know them today started in the late 1970s and early 1980s and have grown as a part of Pharma R&D budgets from 4 percent in the 1990s to close to 50 percent in the mid 2000s. In a previous post on why Pharma needs mobile apps, I briefly mention their potential role in clinical trials. I would like to discuss this in more detail now. The cost of performing clinical trials is increasing significantly. Technology including mobile technology and analytics can decrease these costs, but the challenge is for both business models and the research processes to adapt around them. This presupposes that the technologies can perform trials well. .. Both the European Medicines Agency and the FDA have endorsed centralized monitoring of trials via technology on a real-time basis. .. Recruitment of patients is another aspect of digital technology in clinical trials. Pfizer used social media to recruit patients for a clinical trial of Detrol. One company hosting 200,000 patients in online communities which gather data on 150,000 disease states, PatientsLikeMe has signed agreements with pharmaceutical companies to match patients with trials using its clinical trial search tool. Other advantages of mobile clinical trials, as I see them, include less biased recruitment via crowdsourcing, a dramatic reduction in costs, better medication tracking via pill sensor technology (Proteus Digital Health), and faster reporting of adverse events (which can potentially save lives and stop negative studies earlier via transmission to the Data Safety Monitoring Board), and more timely analytics and trial reporting. In addition, they might lend themselves to more comprehensive or efficient audits, and will strengthen the assistance of caregivers (who can receive and transmit data with/for the patient) in the trial. .. While I do not believe that mobile technology will replace CROs, I do believe that it will significantly reduce costs and improve procedural inefficiencies and accuracy. The digitalization of clinical trial data represented a significant step in improving process and quality of trials. Making it mobile will take it to an even higher level.
David Lee Scher, MD, FACP, FACC, FHRS, is a clinical associate professor of medicine at the Pennsylvania State University College of Medicine,
Via rob halkes
rob halkes's curator insight,
January 16, 2014 5:33 AM
Well, I agree very much with David about the potential and the benefits of using mobile technology in trial studies. Yet, I think that the very patients are entitled to not just that. I know of cases in which patients have been supported and guided on an intensive schedule to their participation in the trial. But, alas, when the trial was over, so the support and guidance disappeared. Why not continue this in the very support at therapy? My take is that both FDA and EMA should take steps to guarantee that services rendered during trials should be continued, by the participating institutes and business of care and research to the services for the participating patients. Isn't that self evident? Please endorse this, by your comments!
|




